
Delusions, which are strong beliefs that defy logical evidence or reality, often emerge when our minds attempt to process the distress linked to mental health issues. While many assume delusions are as unique as fingerprints, they are actually molded by the technologies and cultural contexts of our era.
Just like fashion trends, delusions can change over time and even be influenced or imported from other cultures. Sadly, relying on medical professionals for clarity isn't always effective, as they too can be influenced by similar delusions.
10. The Role of Culture in Shaping Delusions

Our cultural frameworks supply the foundational elements for interpreting and narrating our experiences, including the stories behind our delusions. Those who treat us—be they doctors, priests, or shamans—also play a role in shaping these delusions by categorizing the signs of mental illness.
“Culture can be seen as having a ‘symptom repertoire‘—a collection of physical symptoms that the unconscious mind uses to express psychological struggles,” medical historian Edward Shorter told the New York Times. “In certain periods, symptoms like convulsions, sudden speech loss, or severe leg pain might dominate. In others, issues such as abdominal pain, distorted body weight perceptions, or overwhelming fatigue might serve as metaphors for emotional distress.”
For instance, some men in Southeast Asia may experience koro, a condition where they believe their genitals are shrinking despite no physical abnormalities. Similarly, in the Middle East, individuals with zar are thought to be under the influence of spirits, leading to episodes of shouting, laughing, and singing as expressions of their emotional detachment.
Mass delusions are shaped in similar ways. For example, repressed nuns from the 15th to the 19th centuries often experienced collective delusions. Influenced by widespread beliefs in demonic possession and strict religious practices, these women exhibited hysterical behaviors such as cursing, exposing themselves, and making suggestive movements. While priests performed exorcisms, some nuns faced imprisonment or execution.
Between the 18th and early 20th centuries, harsh working environments in Western factories led to unusual movements, seizures, and neurological issues among groups of workers.
As the 20th century unfolded, mass delusions shifted toward anxiety-driven symptoms tied to environmental and wartime fears. Following the deadly use of poison gas in World War I, which claimed 90,000 lives, Americans developed a deep-seated fear of gas. In the 1930s, numerous residents in rural Virginia believed their homes had been targeted with toxic gas overnight. Investigations later revealed the causes ranged from harmless flatulence to blocked chimney flues.
The anthrax scare after the 9/11 attacks also triggered numerous false alarms across the US. For instance, a student and teacher reported chemical burns on their arms after opening a letter in October 2001, but no harmful substances were found in the envelope.
9. The Impact of Technology

While feelings of loneliness, alienation, and anxiety that fuel delusions are timeless, their expression evolves to reflect cultural and technological shifts. Before the late 19th century, delusions of control or persecution often revolved around witchcraft and supernatural forces. This shifted as technologies like the telegraph, telephone, radio, TV, electricity, X-rays, lasers, and the Internet gained prominence.
Delusions rarely revert to past themes unless a specific era holds particular significance for an individual. Today, delusions frequently involve fears of being controlled or persecuted through computers and the Internet, rather than through radio waves, as was common in the 1940s.
A 2010 study revealed that excessive Internet use can lead to sudden psychotic episodes. In three distinct cases, women aged 30–50 with no prior serious mental health issues developed delusions and hallucinations after spending many hours daily online. Each woman had experienced dissatisfaction in past relationships and was engaged in purely online romances. Over time, they lost touch with reality, with one woman even believing she could physically feel her online partner’s touch despite never meeting him. All required antipsychotic medication to recover.
In another instance, a man became convinced that his computer was being used to implant thoughts in his mind and poison him through his keyboard.
Historically, new materials were the cutting-edge technologies of their time. For example, the glass delusion became widespread in Europe, peaking in the 1600s. It reportedly began with French king Charles VI, who feared betrayal and assassination. During episodes, he would freeze, believing he was made of glass and could shatter. He even wrapped himself in blankets to protect his body. Psychologists suggest this delusion reflects fears of fragility or social shame. In a 1960s case, a Dutch man told the BBC that people saw through him like glass in a window, stating, “You don’t see the glass, but it’s there. That’s me—I’m there, and I’m not there, like the glass in the window.”
8. The Role of Media and Entertainment in Shaping Delusions
While the extent of the panic caused by Orson Welles’ 1938 War of the Worlds radio broadcast remains debated, it’s clear that media and entertainment have influenced delusional beliefs. Over the years, we’ve witnessed how topics in the media can shape collective delusions.
In 2008, Australian doctors documented the first case of climate change delusion. A 17-year-old patient, convinced of impending ecological collapse, refused to drink water, fearing it would lead to the deaths of millions. This sparked public debate, with critics blaming the media for sensationalizing climate change and contributing to his delusion. One blog even claimed, “Al Gore Is Literally Driving People Crazy.” However, delusions often serve as a way for individuals to express their anxieties through narratives that reflect contemporary concerns.
Entertainment also plays a significant role in fueling delusions. Some individuals believe they are characters in video games, while others are convinced they have romantic ties with or are being targeted by famous celebrities.
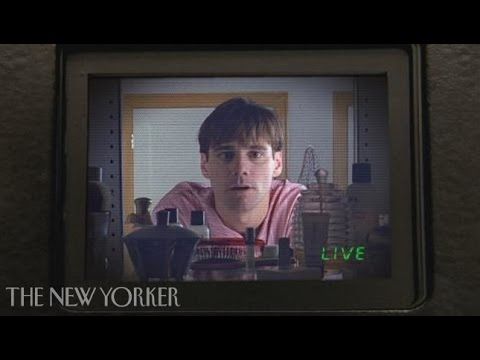
The Truman Show Delusion (TSD), inspired by a film about a man discovering his life is a reality TV show, reflects modern anxieties about surveillance and control. With so much of our lives being recorded unknowingly and the growing popularity of reality shows, some people now believe they are the stars of their own unscripted series.
“[Patients feel] as though their family might be following a script, with cameras constantly monitoring them, leaving no room for privacy,” psychiatrist Dr. Joel Gold explained to NPR. “For most, this was deeply unsettling. A small group, however, felt a thrill, believing they were the most famous individuals on the planet. But even for them, the delusion eventually became too much to bear.”
Gold highlights that TSD stands out in a significant way. Unlike most delusions, which center on a single unreal aspect of life—like alien abduction—TSD engulfs the patient’s entire reality. To them, nothing feels genuine.
7. The Global Spread of America’s Delusions

In his book Crazy Like Us, Ethan Watters contends that the US has spread its perspective on mental illness to other nations, even when American definitions of mental health conditions don’t align with the symptoms observed in those cultures.
While a single antibiotic can treat the same bacterial infection globally, this one-size-fits-all approach often fails in mental health care. Watters raises concerns about whether we’re aiding or harming patients by ignoring the cultural contexts that shape their delusions and mental health experiences.
“This doesn’t imply that these illnesses or the suffering they cause are imaginary, or that individuals intentionally mold their symptoms to fit cultural expectations,” Watters explains. “It means that mental illness is rooted in the mind and cannot be fully understood without considering the ideas, habits, and predispositions—the unique cultural frameworks—of the mind it inhabits.”
Following the 2004 tsunami in Sri Lanka, American mental health professionals arrived to assist, expecting to see symptoms of post-traumatic stress disorder (PTSD). However, this assumption clashed with local cultural norms. “Nightmares and flashbacks weren’t the primary concerns for most Sri Lankans,” trauma specialist Gaithri Fernando told the New York Times. “The most profound psychological wounds were tied to the disruption or loss of their roles within their communities.”
While Americans focused on individual mental trauma, Sri Lankans emphasized the impact on their social structures. Psychology professor Ken Miller noted similar patterns in Afghanistan, Bosnia, and Guatemala, where PTSD symptoms didn’t align with the trauma caused by war. Exporting American psychiatric practices to certain countries, regardless of their development, can create a cultural mismatch as stark as sending Namibian witch doctors to treat Americans after 9/11.
If anxiety about global changes can lead to delusions, are American psychiatrists exacerbating the issue by imposing their methods on how other cultures define and manage stress? As we’ll explore, American psychiatric practices don’t always result in better treatments or outcomes for patients, nor are they always aligned with the patient’s best interests.
6. The Delusions of the Doctors Who Diagnose Us

Some physicians may think they assess and treat mental illness with complete objectivity. This belief is particularly strong among certain US practitioners, who assume that while other nations have cultural delusions, American doctors address genuine brain disorders using scientific methods.
However, US doctors are just as influenced by cultural biases and delusions in their approach to mental health as anyone else. Despite their advanced imaging technology and medications designed to alter brain chemistry, they often fail to recognize this. As Ethan Watters notes, “All mental illnesses, including depression, PTSD, and even schizophrenia, can be just as shaped by cultural beliefs and expectations as historical conditions like hysterical-leg paralysis, the vapors, or zar.”
As demonstrated in Sri Lanka, Western doctors often assume they know which life events trigger mental illness and are confident in their treatment methods. Many American doctors also advocate for discussing personal traumas, analyzing them, and expressing emotions openly. They operate under the belief that people are psychologically fragile. However, many cultures, including those in developed nations like Australia, don’t share these perspectives, which can render American treatments ineffective.
This isn’t to say the US hasn’t developed treatments that could benefit patients elsewhere. However, American doctors often appear unwilling to consider alternative approaches to mental health care.
5. Improved Mental Health Outcomes in the Developing World

Starting in the early 1970s, the World Health Organization (WHO) carried out three global studies on schizophrenia patients, spanning approximately 30 years. The findings revealed that relapse rates for schizophrenia patients in Europe and the US were up to 67 percent higher compared to those in developing nations.
This sparked extensive debate about the reasons behind the disparity. One hypothesis suggests that schizophrenia patients in some developing countries are treated more compassionately and remain better integrated within their social groups. Anthropologist Juli McGruder, who studied schizophrenia patients and their families in Zanzibar, noted that delusions are often attributed to spirit possession. “In Muslim and Swahili cultures, spirits aren’t exorcised in the Christian sense of driving out demons,” McGruder explained to the New York Times. “Instead, they are appeased with food and gifts, celebrated with music and dance. They are calmed, settled, and their harm is minimized.” Patients are viewed as temporarily ill rather than permanently changed. When symptoms subside, they can reintegrate into society, at least temporarily.
In contrast, Western cultures place a high value on self-control and mastery over one’s circumstances, which conflicts with the nature of mental illness. Unlike developing nations that accept spirit possession, Western families often expect their loved ones to recover through sheer willpower. This leaves patients feeling more isolated and less likely to return to work. Mental illness is frequently seen as a lifelong condition.
Some researchers argue that the WHO studies were flawed in their methodology. They also contend that the prognosis for schizophrenia patients in developing countries has deteriorated significantly in recent years, prompting calls for new research.
Other studies suggest that variations in medication use explain the outcomes of the WHO research. These researchers concluded that reducing reliance on antipsychotic drugs leads to better long-term outcomes for schizophrenia patients worldwide.
Despite this, none of the studies indicated that Western medicine delivered significantly better outcomes for schizophrenia patients.
4. The Commercialization of Mental Illness

One key reason the US is so determined to export its definitions and treatments for mental illness, including delusions, is the pursuit of pharmaceutical profits. A notable example occurred in Japan at the start of the 21st century, when drug companies persuaded the public that they suffered from mild depression, termed kokoro no kaze, or “cold of the soul.” Naturally, these companies offered costly antidepressants as the solution.
Before this, Japan’s medical community only recognized severe depressive disorders. With a suicide rate twice that of the US, Japan clearly faced mental health challenges. The average hospital stay for mental illness was around 390 days, far exceeding the US average of under 10 days. Officially, mild depression wasn’t acknowledged in Japan. However, after the drug companies launched their media campaign, visits to doctors for depression surged by nearly 50 percent in just four years.
“I could take you anywhere in the world, and you’d easily identify severely depressed individuals in entirely different cultures,” psychiatry professor Arthur Kleinman told the New York Times. “But mild depression is a completely different matter. It allows us to categorize a wide range of experiences as depression.” The line between moodiness and depression is often blurred, making it possible that the Japanese began labeling non-disease conditions as mild depression. They were repeatedly told that medication was the solution.
A 39-year-old man, Naoya Mitake, was prescribed various antidepressants for two years to address insomnia and fatigue. Drug company campaigns had convinced him that his symptoms had a chemical basis requiring medication. However, the treatment never fully worked. Eventually, he discovered his own remedy: fasting.
As Japanese psychiatrist Yutaka Ono explained to the New York Times, “[The drug companies] launched an aggressive campaign about mild depression, featuring a cheerful young woman who says, ‘I visited a doctor, and now I’m happy.’ But depression isn’t that simple. If it were, it might not even be depression.”
Despite this, antidepressant sales in Japan increased fivefold between 1998 and 2003, shortly after the marketing campaigns began.
3. The Gradual Disappearance of Our Delusions
In Western culture, we often believe that our scientific approach to mental health makes us more advanced than practitioners from other cultures or historical periods. This sense of superiority leads us to view past treatments with a mix of mockery and pity.
Today, we rely on the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM), often called the “Bible of psychiatry.” It outlines symptoms of disorders recognized as psychiatric illnesses in the US, effectively defining what society considers normal or abnormal behavior—what allows us to live freely and what might lead to medication or even confinement.
However, the DSM isn’t as objective as we might assume. US psychiatrist Daniel Carlat notes that psychiatrists have been among the top recipients of funding from drug companies for years because “our diagnoses are subjective and flexible, and we lack clear reasons for choosing one treatment over another.” Carlat also admits that he earns 80 percent more per hour by prescribing medications rather than offering talk therapy, so he focuses solely on drug prescriptions.
“Patients often see psychiatrists as masters of neurotransmitters,” he explains, “capable of selecting the perfect medication for any chemical imbalance. This inflated view of our abilities has been promoted by drug companies, by psychiatrists themselves, and by patients’ understandable desire for effective treatments.”
Psychiatrists evaluate patients by matching their symptoms to conditions listed in the DSM. The more symptoms align, the more medications may be prescribed. This labeling system gives patients a sense of being cared for while generating revenue for the medical field. However, as Carlat points out, this doesn’t necessarily mean psychiatrists fully understand the underlying issues.
If this is how our culture defines delusions, we can only hope they diminish sooner rather than later. It also prompts us to wonder how future generations will perceive our delusions and the doctors who treated them.
2. The Debate Over Chemical Imbalance
Medications for psychosis rank among the top-selling drugs in the US. Yet, evidence increasingly suggests these drugs don’t address a chemical imbalance causing mental illness. In fact, early psychiatric drugs like Thorazine, Miltown, and Marsilid were originally developed to fight infections. When they were found to alleviate mental symptoms, researchers noted their impact on brain chemistry. The drugs weren’t designed to correct chemical imbalances; the theory was developed to justify their use. Decades of research have failed to validate the chemical imbalance hypothesis across various classes of psychiatric medications.
Nevertheless, the critical question remains: do these drugs actually work? Irving Kirsch, a UK psychologist, analyzed published clinical trial results for depression treatments and initially discovered that placebos were about 82 percent as effective as antidepressants. His most significant finding, however, was that drug companies often suppress unfavorable trial results, allowing them to conduct repeated tests until they achieve the desired outcomes. Kirsch concluded that antidepressants showed no meaningful clinical advantage over placebos. While there was a minor statistical difference, it wasn’t substantial enough to impact real-world treatment.
Kirsch also found that non-antidepressant substances—such as sedatives, thyroid hormones, stimulants, opiates, and even some herbal remedies—were equally effective in alleviating depression symptoms. When examining high-dose placebos that produced side effects, he observed similar outcomes. This led him to conclude that side effects might convince patients that medications are more effective than side-effect-free placebos.
While Kirsch’s study is just one analysis of a complex issue, and no one should stop taking medication based solely on it, it does raise important questions about drug efficacy. Further research is needed to explore this topic in greater depth.
1. Our Connection to Our Delusions
Stanford anthropologist Tanya Luhrmann studied how individuals with psychotic disorders interacted with the voices (auditory hallucinations) they experienced. In the US, these voices were often perceived as hostile and aggressive. In contrast, in Ghana and India, the voices were frequently seen as harmless or even playful.
Luhrmann argues that American doctors should place greater emphasis on auditory hallucinations and cultural variations in psychiatric conditions. “Our research revealed that people with severe psychotic disorders in different cultures have distinct voice-hearing experiences,” she noted. “This implies that how individuals engage with their voices influences what they hear, which could have significant clinical implications.”
In a study involving 60 adults with schizophrenia—20 each from Ghana, India, and the US—Luhrmann found that participants in all three countries experienced both positive and negative voices, whispers, and unidentified hissing sounds. However, the key difference lay in how they interpreted these experiences. All US patients described negative encounters, viewing the voices as symptoms of a brain disorder. They perceived the voices as hostile and violent, often likening the experience to warfare.
About half of the Indian participants heard relatives guiding them to complete tasks, sometimes interpreting the voices as playful or entertaining. Most did not attribute their hallucinations to a brain disease. Similarly, Ghanaian patients, who culturally believe spirits can communicate, did not see the voices as a psychiatric issue. Half described their experiences positively, and 80 percent believed they had heard from God.
Luhrmann suggests these differing reactions reflect cultural values. Americans prioritize independence, individuality, and control, while Ghanaians and Indians define themselves through their relationships with others. This insight could lead to innovative schizophrenia treatments, such as identifying patients’ voices and building relationships with them.
“The issue isn’t hearing voices,” Dr. Marius Romme, founder of the advocacy group Intervoice, explained to The Atlantic, “but the struggle to manage the experience.” Dr. Dirk Corstens, Romme’s colleague, also advocates for reducing the use of medication in treating psychosis, as it often causes more harm than benefit.