
 While obesity is a widespread health crisis, could there be scenarios where it offers advantages? Peter Dazeley / Getty Images
While obesity is a widespread health crisis, could there be scenarios where it offers advantages? Peter Dazeley / Getty ImagesApproximately 65% of Americans are either overweight or obese, with the Centers for Disease Control labeling obesity as a national epidemic. The NIDDK/NIH reports that obesity-related healthcare costs exceed $117 billion each year. Obese individuals face a 50 to 100% higher risk of early death compared to those with normal weight. Obesity also increases the likelihood of conditions such as hypertension, heart disease, and type-2 diabetes. However, recent research indicates that obese individuals with chronic illnesses may have higher survival rates than their normal-weight counterparts. This phenomenon is known as the obesity paradox. Before indulging in extra treats or delaying dietary changes, let's delve deeper into what obesity entails.
Obese individuals carry an excessive amount of body fat, while overweight individuals have surplus body weight, which includes fat, muscle, and bone. Typically, women possess more body fat than men. Women with over 30% body fat and men with over 25% body fat are classified as obese.
Body fat can be measured using advanced techniques such as X-ray absorption and underwater weighing, which rely on the principle that fat tissue differs in density from muscle or bone. However, these methods are not suitable for regular medical check-ups. Instead, healthcare professionals often rely on simpler approaches like assessing height, weight, and skin-fold thickness.
The most widely used and accessible way to estimate obesity is through the body mass index (BMI). BMI calculates the ratio of weight to height using the following formula:
BMI = weight (lb) / [height (in)] x 703 (English measurements)
BMI = weight (kg) / [height (m)] (metric measurements)
For instance, a woman who is 5 feet 5 inches tall and weighs 150 pounds would have a BMI of 25. Based on BMI classifications, she would be considered overweight but not obese.
- Less than 18.5 = underweight
- 18.5 to 24.9 = normal weight
- 25 to 29.9 = overweight
- More than 30 = obese
Numerous online charts utilizing BMI calculations are available to help you determine your weight category.
 Image courtesy FDA
Image courtesy FDAObesity impacts men and women across all racial and ethnic groups, though women tend to have higher obesity rates than men. In the U.S., African-Americans exhibit the highest obesity rates, followed by Mexican-Americans and non-Hispanic whites. Approximately 11 to 28 percent of children are affected by obesity, mirroring the same racial and ethnic trends. Obesity elevates the risk of conditions such as hypertension, cardiovascular disease, stroke, cancer, gallbladder disease, and diabetes. Obese individuals often have elevated levels of cholesterol and lipids in their bloodstream, contributing to the formation of atherosclerotic plaques in blood vessels. This increases the likelihood of high blood pressure, heart attack, and stroke, making obesity a significant risk factor for cardiovascular disease.
Next, we'll explore how researchers uncovered the obesity paradox.
Obesity Paradox Research
 Research on the obesity paradox reveals that individuals with chronic illnesses who are obese often have longer lifespans compared to healthier individuals.
Mytour
Research on the obesity paradox reveals that individuals with chronic illnesses who are obese often have longer lifespans compared to healthier individuals.
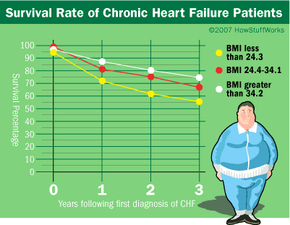
MytourIn 2001, A. Mosterd and his team in the Netherlands investigated the outcomes of patients with heart failure. Analyzing over 5,000 patients, some with heart failure, they discovered that those with lower BMIs and blood pressure experienced higher in-hospital mortality rates than those with higher BMIs. Their findings aligned with a 1993 Massachusetts study, and since then, at least eight additional studies have corroborated these results. Despite obesity being a known risk factor for heart failure, it appears that obese patients with heart failure may fare better.
The obesity paradox isn't limited to heart failure. Patients with chronic kidney disease, often undergoing hemodialysis to filter impurities from the blood, face a 20% annual mortality rate from cardiovascular issues. Research from UCLA Medical Center indicates that dialysis patients with higher BMIs have better survival rates than those with lower BMIs [source: Kalantar-Zadeh].
In summary, the obesity paradox suggests that while obesity is a significant risk factor for cardiovascular diseases (such as hypertension, congestive heart failure, and coronary artery disease) and chronic kidney disease, it may also be linked to improved survival rates in patients with these conditions. If validated, this could reshape how doctors manage chronic disease patients, potentially reducing the emphasis on diets and weight loss.
So, what causes the obesity paradox? We'll explore this on the next page.
It’s crucial to recognize that the obesity paradox has been identified through statistical analyses of extensive datasets in all reported studies. These analyses reveal correlations between factors retrospectively but do not establish causation. Only well-designed animal studies or clinical trials, where variables can be tightly controlled, can demonstrate cause and effect.
Obesity Paradox Explanations
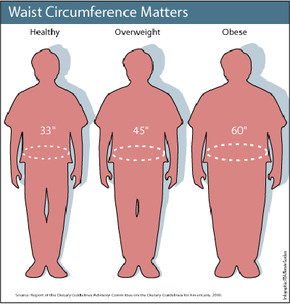 Photo courtesy FDA
Photo courtesy FDAThe medical community has responded with mixed reactions to the obesity paradox. Many physicians and researchers remain skeptical, as the findings contradict expectations based on the general population. Experts from the University of Texas School of Public Health and Baylor Medical College reviewed numerous studies on the obesity paradox and proposed six potential explanations for the phenomenon, while also highlighting reasons to approach the findings with caution [source: Habbu].
- The sample sizes in studies reporting the obesity paradox were often small. Can these findings be generalized to larger populations?
- Statistical methods reveal correlations between factors but do not establish causation. Thus, the results might not reflect reality.
- In numerous studies, congestive heart failure was diagnosed based on clinical symptoms (difficulty breathing, swelling in limbs) rather than laboratory tests such as echocardiography, cardiopulmonary testing, or cardiac catheterization.
- The clinical criteria used to diagnose congestive heart failure have not been validated for obese individuals and may not be suitable.
- In studies where lab tests were conducted, obese patients exhibited slightly better heart function (pumping efficiency, oxygen delivery) compared to normal or underweight patients.
- This suggests that obese patients might be in better health regarding CHF or at earlier stages of the disease than their normal/underweight peers, leading to higher survival rates.
- Congestive heart failure (and chronic kidney disease) is a wasting condition. Patients often lose weight (fat, muscle mass) as the disease progresses. This raises two possibilities:
- Obese patients might be healthier or in earlier stages of these chronic conditions. Low BMIs in chronic disease patients result from the disease's wasting nature, not intentional weight loss through diet or exercise. None of the studies differentiated between intentional and unintentional weight loss.
- Obese patients may possess greater metabolic reserves than their normal or underweight counterparts.
- Few studies examined extreme obesity (BMI over 35). In those that did, extremely obese individuals did not show better survival rates than underweight patients. This suggests survival probabilities might follow a U-shaped curve, with normal and overweight patients faring better than those at the extremes—underweight and extremely obese.
- Recent studies have questioned whether BMI is the optimal measure for obesity. Waist circumference or waist-to-hip ratios might be more accurate indicators, as abdominal fat is more strongly linked to obesity-related risks than fat stored elsewhere. [source: Romero-Coral].
On the next page, we'll explore additional explanations and criticisms of the obesity paradox theory.
Obesity Paradox Criticisms
 Medical professionals remain uncertain about the validity of the obesity paradox.
Medical professionals remain uncertain about the validity of the obesity paradox.While there are numerous reasons to doubt the obesity paradox, UCLA researchers have proposed some biological explanations for it [source: Kalantar-Zadeh].
- The harmful effects of obesity develop more slowly than those of chronic diseases like heart failure or kidney disease. As a result, the impact of wasting diseases can be fatal much quicker than the consequences of obesity.
- In both CHF and chronic kidney disease, malnutrition and inflammation are prevalent. These factors alone can decrease patient survival rates. Thus, weight gain might signal better nutrition and, consequently, higher survival chances for obese patients.
Dr. Kalantar-Zadeh suggests that dietary restrictions for CHF and chronic kidney disease patients could be detrimental. He supports a "reverse epidemiology" approach to managing these conditions.
The obesity paradox has been noted in various clinical settings, such as CHF and chronic kidney disease, but physicians and researchers remain uncertain about its validity. Few have proposed biological explanations for the paradox, and no direct animal studies or clinical trials have established cause-and-effect relationships.
Given the current evidence, we cannot definitively conclude that the obesity paradox is real, nor is there enough justification to change treatment protocols for CHF and chronic kidney disease patients. However, many scientists believe further research is essential to clarify the paradox, as it could influence future treatment strategies.
Dr. Kalantar-Zadeh and his team argue that risk factors for the general population may not apply to obese individuals. The obesity paradox exemplifies this concept, termed reverse epidemiology. They contend that imposing dietary restrictions on obese patients with chronic diseases could be harmful and point to several conditions where similar paradoxical phenomena have been observed [source: Kalantar-Zadeh].