
1. Causes of Sciatic Nerve Pain
In traditional medicine, the causes of sciatic nerve pain are usually attributed to three main factors: wind, dampness, and cold, which lead to blockages in the body’s circulation, causing pain in the lower back and waist area.
According to modern medicine, sciatic nerve pain is primarily caused by damage to the disc or joints in the lower back, which puts pressure on the sciatic nerve.
Specifically, six factors can lead to sciatic nerve pain:
- Herniated disc: The leading cause of sciatic pain occurs when a disc between two vertebrae in the lower back is damaged or aged, causing the soft core to push out and compress the sciatic nerve.
- Spinal stenosis: Common in people over 60 years old. Spinal degeneration over time narrows the spinal canal, creating pressure on the hips, particularly the hip nerves and sciatic nerve.
- Spinal tumors: Tumors in the spine or surrounding nerves create pressure that compresses the nerve roots, which can lead to sciatic nerve pain if located in the lower back.
- Spinal injury: Accidents, falls, or strong impacts can cause inflammation, fractures, or herniated discs, all of which can compress the sciatic nerve.
- Psoas muscle syndrome: A less common condition where the psoas muscle, located near the lower spine and hip, spasms and compresses the sciatic nerve.
- Other causes: Pressure from pregnancy, complications from conditions like diabetes, constipation, cardiovascular issues, or infections can also lead to sciatic nerve pain.

2. What Are the Symptoms of Sciatic Nerve Pain?
Symptoms of sciatic nerve pain include:
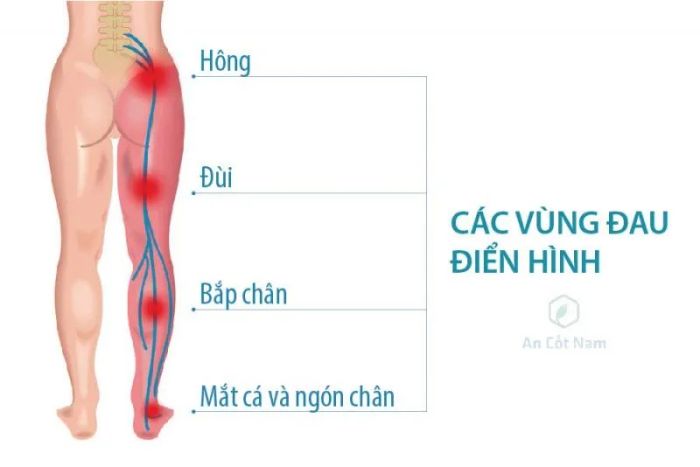
- Pain along the path of the sciatic nerve, starting from the lower back and radiating to the outer thigh, front of the lower leg, outer ankle, and extending to the toes. Depending on the location of the nerve damage, the clinical presentation may vary: damage to the L4 root causes pain to radiate to the back of the knee, damage to the L5 root causes pain to spread to the top of the foot and end at the big toe, and L5 root damage can cause pain to extend to the sole of the foot and end at the pinky toe. In some cases, there may be no pain in the lower back, but pain may only occur along the leg.
- The pain radiating from the lower back (lumbar) to the buttocks and down the back of the leg is a hallmark sign of sciatic nerve pain. You may experience discomfort along almost the entire length of the nerve, but it tends to follow a path from the lower back to the buttocks, down the back of the thigh, and calf.
- The pain can vary significantly, from mild discomfort to sharp, stabbing, or intense pain. Sometimes it may feel like a jolt or electric shock. Coughing or sneezing can exacerbate the pain, and prolonged sitting can worsen the symptoms. Usually, only one side of the body is affected.
- Some individuals may also experience numbness, tingling, or muscle weakness in the affected leg or foot. You may experience pain in one area of the leg and numbness in another.
3. How to Prevent Sciatic Nerve Pain
It is not always possible to prevent sciatic nerve pain, and it can recur. However, the following practices may play an important role in reducing the likelihood of developing sciatic nerve pain:
- Engage in regular physical exercise
- Maintain proper sitting posture: choose a chair that provides good lower back support, has armrests, and a swivel base. Consider placing a cushion or rolled towel behind your lower back to maintain its natural curve.
- Use proper body mechanics: avoid overloading the lower back with tasks like lifting heavy objects. Instead, use your legs to lift, keep your back straight, and bend only at the knees. Avoid lifting and twisting your back at the same time.

4. Methods for Diagnosing Sciatic Nerve Pain
To accurately diagnose sciatic nerve pain, a doctor will rely on both clinical and paraclinical assessments.
Clinical diagnosis of sciatic nerve pain
The doctor will ask for detailed information about the symptoms the patient is experiencing, along with some physical tests such as:
- Valleix pain point system and a positive straight leg raise test.
- Positive Lasegue's sign.
- Chavany's sign; Bonnet's sign.
- Bone reflexes: testing the patellar reflex for weakness or total loss in case of L4 root damage; testing the Achilles reflex for weakness or loss in case of S1 root damage.
Paraclinical diagnosis of sciatic nerve pain
The following tests may be used:
- X-ray: This technique has little diagnostic value in identifying the cause of the condition, but it can help identify bone-related issues such as spinal degeneration, spondylolisthesis, tuberculosis of the spine, ankylosing spondylitis, or spinal stenosis.
- Magnetic Resonance Imaging (MRI): An MRI provides precise images of the damage location and the degree of compression, which helps doctors decide on appropriate treatment.
- CT Scan: If a patient cannot undergo an MRI, a CT scan may be recommended.
- Electromyography (EMG): By measuring the electrical activity generated by nerves and muscle response, this test helps assess the extent of nerve root damage.

5. Treatment for Sciatica
Principles for treating sciatica:
- Treat based on the underlying cause (most commonly lumbar disc herniation).
- Relieve pain and promote quick recovery of mobility.
- Medical treatment for mild to moderate cases.
- Surgical intervention for complications affecting movement or sensation.
- For sciatica caused by malignancy: decompression of the spine along with specialized treatment.
Medical Treatment
- Rest: sleep on a firm mattress, avoid sudden, strong movements, heavy lifting, and prolonged standing or sitting.
Medications
- Pain relievers, depending on the severity of pain, including paracetamol, NSAIDs (be cautious of their side effects on the digestive system, heart, liver, and kidneys). Consider combining them with stomach protectants and acid reducers to reduce ulcer risks.
- If pain is severe, opioid medications like morphine may be required.
- Muscle relaxants
- Neuropathic pain relievers
- Vitamin B complex supplements
- Corticosteroid injections: targeted at nerve roots in sciatica cases, which can be administered under fluoroscopic or CT guidance.
Physical Therapy
- Once the acute pain improves, physical therapy professionals may create a rehabilitation plan to prevent future injuries, including exercises to improve posture, strengthen back muscles, and increase flexibility.
- Massage therapy.
- Therapeutic exercises: stretching the spine, light hanging exercises, swimming, and specific back exercises to strengthen the spine.
- Wearing a back brace to prevent excessive load on spinal discs.
Surgical Treatment
- Indicated when medical treatment fails or in severe cases with nerve compression (cauda equina syndrome, spinal stenosis, lower limb paralysis, muscle atrophy). Surgical approaches vary depending on disc herniation, spondylolisthesis, or compressive tumors, including minimally invasive, radiofrequency, microdiscectomy, or open surgeries. Common procedures include:
- Discectomy: removing part of the herniated disc causing nerve compression, typically after 3 months of ineffective pain management. Early surgery is advised for severe mobility restrictions and sensory disturbances.
- Laminectomy: for sciatica due to spinal stenosis, though it may cause spinal instability and risk of recurrence.
- For spondylolisthesis causing severe nerve compression, spinal fusion using screws and rods is recommended.
Supportive Treatment
- Cold compress: initially, use an ice pack on the painful area for 20 minutes several times a day, wrapped in a clean towel.
- Heat compress: after 2-3 days, apply heat to the affected area using a warm pack, heating lamp, or low-temperature heating pad. Alternate between warm and cold packs if pain persists.
Other Treatments
- Alternative therapies commonly used for back pain include:
- Acupuncture: practitioners insert thin needles into specific points on the body, with some studies suggesting it may reduce back pain, though not all studies support its effectiveness. Always choose a licensed practitioner for proper training.
- Chiropractic adjustments: spinal manipulation is a form of therapy that aims to restore spinal movement and alleviate pain. It is considered as effective and safe as conventional treatments for lower back pain, though it may not always be suitable for pain relief.

6. What is Sciatica?
Sciatic Nerve, also known as the largest nerve in the body, runs from the lower back to the back of both legs, passing through the sacral vertebrae. It controls the movement of the lower back and legs.
Sciatica refers to the pain that travels along the path of the sciatic nerve. The pain usually starts in the lower spine and radiates down to the outer thigh, calf, and possibly to the outer ankle or toes, depending on the location of the nerve damage.
This condition is quite common, especially among individuals aged 30 to 50, and the primary cause is often disc herniation that compresses the nerve, leading to inflammation and pain (about 80% of cases). Other, less common causes include trauma, vertebral disc inflammation, or spinal body injuries, which can also trigger sciatica pain.

7. Who is at risk for Sciatica?
People suffering from sciatica are mostly older adults, those with long-term diabetes, and individuals with obesity. You can reduce your risk of developing this condition by minimizing certain risk factors.
Below are some factors that increase the risk of sciatica:
- Age: age-related changes in the spine, such as disc herniation and bone spurs, are the most common causes of sciatica.
- Obesity: excess body weight can put additional stress on the spine, contributing to spinal changes that cause sciatica.
- Occupation: jobs that involve twisting the back, lifting heavy objects, or long hours of driving may play a role in sciatica, although there is no conclusive evidence supporting this link.
- Prolonged sitting: people who sit for extended periods or lead a sedentary lifestyle are more likely to develop sciatica than those who are more active.
- Diabetes: increases the risk of nerve damage.


8. Is Sciatica Dangerous?
Sciatica is not life-threatening; typically, the pain associated with sciatica will subside on its own. However, the complications caused by sciatica can be quite uncomfortable for the patient and may lead to a decrease in mobility function.
When sciatica becomes chronic, the pain may persist continuously and significantly impact the patient's quality of life. Additionally, if the nerve is severely compressed, it can affect the muscles, causing weakness and muscle wasting, such as in the case of foot drop (also known as peroneal nerve damage or dropped foot). This condition results in numbness and the inability to walk properly.
Worse still, sciatica can lead to permanent nerve damage, which can result in a complete loss of sensation in the leg.
If sciatica is not treated promptly, it can easily develop into a chronic condition, making complete recovery more difficult. The pain may gradually worsen, causing discomfort, irritability, and fatigue. As the condition progresses, it can lead to serious complications such as numbness, loss of leg function, muscle wasting along the path of the sciatic nerve, spinal deformities, and even permanent disability. In severe cases, it may result in incontinence due to disrupted nerve function.
