1. Who is Most Likely to Develop Peripheral Artery Disease?
Approximately 75% of cases show no symptoms. Peripheral artery disease is increasingly prevalent due to rising life expectancy, lifestyle changes, and particularly the growing incidence of cardiovascular risk factors. After the age of 70, around 20% of the population is affected by this condition.
High-risk groups for peripheral artery disease include:
- Smokers
- Individuals with diabetes
- Those with high blood pressure
- People with lipid disorders...
Among these, smoking and diabetes are particularly significant risk factors. If you have even one of these risk factors, it’s important to educate yourself about the disease. As with other conditions, the more you know, the better equipped you are to detect it early.
2. The Importance of Early Detection of Peripheral Artery Disease
Early detection of peripheral artery disease is crucial. Beyond enabling timely treatment for limb ischemia before severe complications like necrosis or amputation arise, individuals with this condition often exhibit atherosclerosis in other arteries, including those supplying the heart and brain. In fact, patients with peripheral artery disease face a 6 to 7 times higher risk of heart attack or stroke compared to those without the disease.
Many patients with peripheral artery disease show no symptoms, especially in the early stages. This often leads to missed diagnoses. Some may only experience calf pain or cramping during prolonged walking. Additionally, many cases are misdiagnosed as arthritis, muscle disorders, or simply signs of aging. Most cases are only identified when advanced symptoms or complications, such as non-healing leg ulcers, severe pain, discoloration, or limb necrosis, appear.
Smokers and individuals with diabetes are at particularly high risk. Effective treatment for peripheral artery disease can alleviate symptoms and reduce the likelihood of amputation, heart attack, or sudden death in the future.

3. How is Peripheral Artery Disease Diagnosed?
In diagnosing peripheral artery disease, intermittent claudication with the described characteristics and clinical examination (such as checking for weak or absent pulses in the limbs) are crucial.
The ankle-brachial index (ABI) is also commonly used. This is a simple, painless test that a doctor can perform in just a few minutes. By comparing blood pressure in the ankle to that in the arm, the doctor can assess the quality of blood flow in the legs. Normally, the ankle pressure should be at least 90% of the arm pressure, but in severe cases of narrowing, it may drop below 50%. Abnormal results may indicate coexisting carotid artery disease.
Additionally, your doctor may recommend further tests, such as:
- Doppler ultrasound
- Multislice computed tomography (MSCT) angiography
- Magnetic resonance imaging (MRI)
- Contrast angiography
4. Treatment of Peripheral Artery Disease
Treatment focuses on two primary goals: Alleviating symptoms and preventing dangerous complications related to arterial disease.
- Quit smoking: Provide support and counseling during follow-ups; develop a tailored smoking cessation plan; avoid environments where smoking is prevalent.
- Improve diet: Support lipid level management and treat lipid metabolism disorders.
- Supervised exercise therapy: Engage in supervised rehabilitation sessions 3-4 times per week, lasting 30-45 minutes, tailored to the patient’s condition and ability. This is recommended to improve symptoms and increase walking distance, with a minimum duration of 12 weeks.
- Manage comorbidities: Control diabetes, hypertension, and coronary artery disease if present. Educate diabetic patients about complications, particularly foot care.
- Pain management: Use appropriate pain relievers or vasodilators based on the disease stage.
- Amputation: Considered in severe cases of necrosis posing systemic risks.
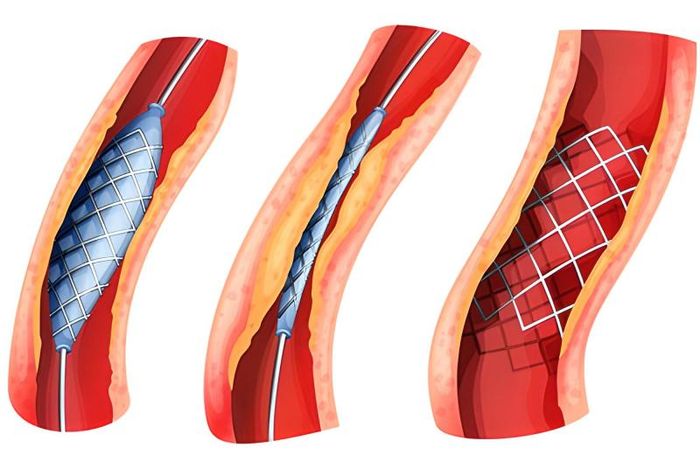
- Revascularization: Recommended for patients with severe complications, unimproved limb ischemia, or uncontrolled risk factors. Key methods include:
5. Preventing Peripheral Artery Disease
Patients with the aforementioned risk factors should undergo peripheral artery screening during each medical visit. Doctors assess limb perfusion by examining skin appearance, comparing temperature, checking pulses, measuring blood pressure on both sides, evaluating sensation, muscle strength, and looking for ulcers or necrosis. If symptoms are unclear or differentiation from other causes is needed, patients may undergo treadmill tests, ultrasounds, or vascular imaging.
The best way to prevent peripheral artery disease is to maintain a healthy lifestyle, such as:
- Avoid smoking
- Effectively manage diabetes if present
- Engage in regular, moderate exercise (30-45 minutes/day) tailored to individual fitness levels under medical guidance
- Control cholesterol and blood pressure
- Limit alcohol and fatty foods while increasing intake of vegetables and fruits
- Maintain a healthy weight
Early detection and prevention of risk factors for peripheral artery disease can also reduce the likelihood of heart attack or stroke.

6. What is Peripheral Artery Disease?
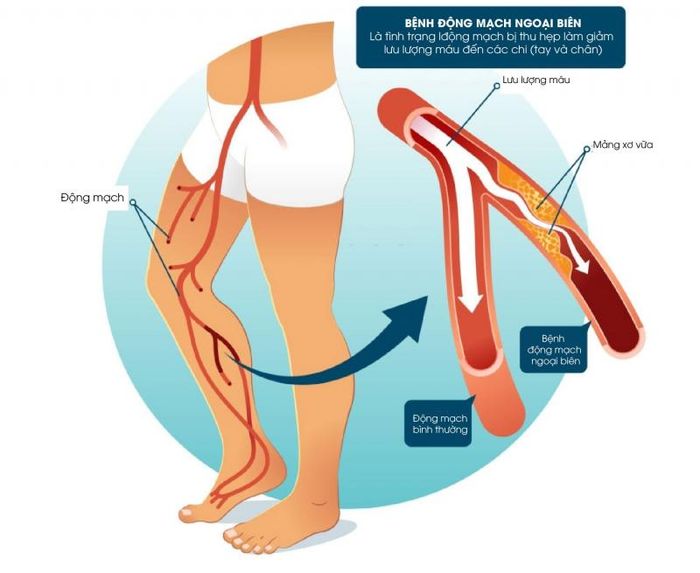
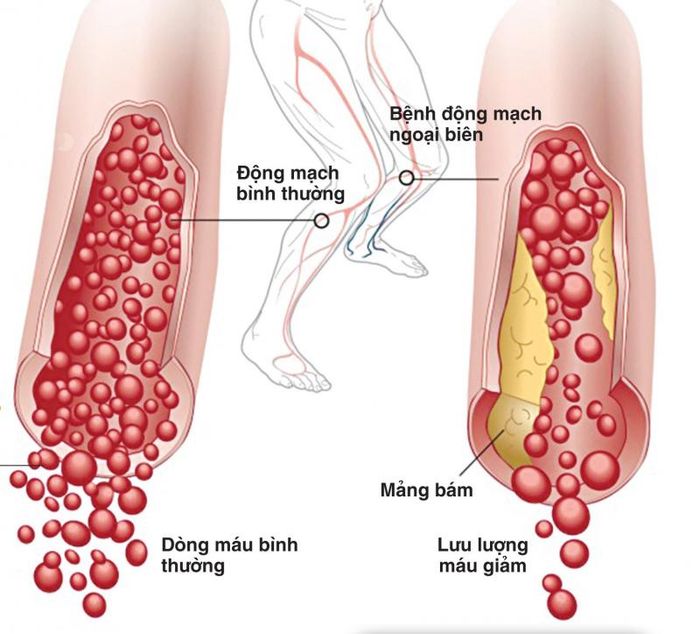
Peripheral artery disease is a condition characterized by the blockage of peripheral blood vessels due to atherosclerotic plaques and blood clots. These arteries do not include those supplying blood to the heart and brain. The most commonly affected areas are the pelvic region, lower limbs, and upper limbs.
Pathologically, the blockage in these vessels is similar to that in coronary or carotid arteries. The difference lies in the areas they supply: coronary arteries feed the heart, carotid arteries supply the brain, while peripheral arteries provide blood to the limbs.
Primary symptoms include intermittent claudication, pain, discoloration, and necrosis with varying characteristics. If not detected and treated early, the disease can lead to tissue ischemia, resulting in limb necrosis, amputation, or joint removal.
7. Symptoms of Peripheral Artery Disease
The most common symptom of peripheral artery disease is cramping in the thighs, hips, or calves during walking, climbing stairs, or exertion. This discomfort typically subsides with rest, even after just a few minutes. The pain arises because muscles require increased blood flow during activity, but narrowed or blocked arteries due to plaque buildup restrict this flow, causing ischemia. At rest, oxygen demand decreases, alleviating the pain. This phenomenon is known as intermittent claudication.
Many people mistake leg pain for a normal part of aging, often attributing it to arthritis, sciatica, or joint stiffness. However, pain from peripheral artery disease usually originates in the muscles (like the calves) rather than the joints. In diabetic patients, this symptom may be masked by neuropathic pain or numbness in the feet or thighs, a common complication of diabetes.
Severe symptoms of peripheral artery disease include:
- Persistent leg pain even at rest.
- Non-healing wounds on the toes or feet.
- Necrosis of the feet or toes.
- The affected leg feeling colder than the unaffected leg or other parts of the limb.

8. Causes of Peripheral Artery Disease
Peripheral artery disease is caused by the following factors:
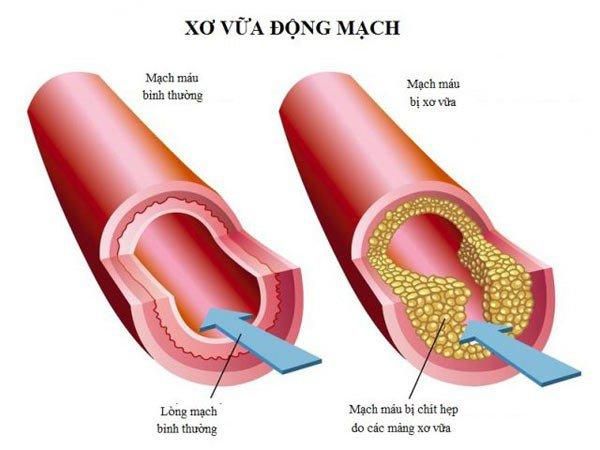
Atherosclerosis
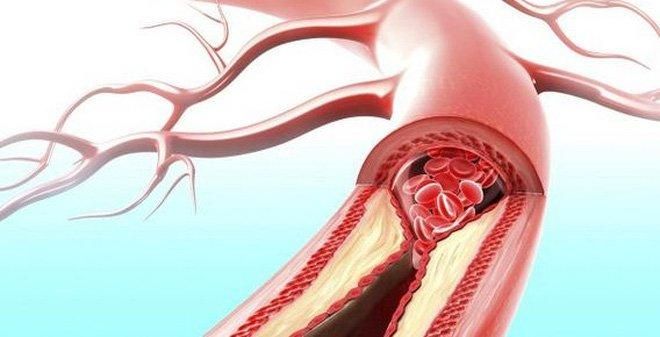
The primary cause of peripheral artery disease is narrowing or blockage due to atherosclerotic plaques. The arterial walls thicken from the accumulation of fat and other substances, forming plaques that narrow the lumen and can completely obstruct blood flow. While atherosclerosis is often associated with the heart, it can reduce blood flow to various parts of the body, particularly the limbs.
Vasculitis
This is a less common cause. Vasculitis occurs due to inflammation from injuries, abnormal muscle or ligament structures, or exposure to radiation.