1. Complications of Heart Attacks
Surviving a heart attack is a stroke of luck, but this is just the beginning. The patient will continue treatment and face the risk of sudden death during the first 3 weeks after the event due to arrhythmia, heart rupture, pulmonary embolism, brain embolism, pulmonary edema, or cardiac shock. After this period, risks start to diminish, but long-term consequences remain a challenge. Thus, during the early stages, both the patient and their caregivers must remain vigilant for any unusual signs to report to doctors and avoid risks.
Early complications:
- Sudden death: 10% of heart attack cases result in sudden death. This is the most severe complication that may arise during the first week after the attack. It is caused by ventricular fibrillation, rapid ventricular rhythm, heart rupture, pulmonary embolism, or acute circulatory failure.
- Arrhythmias: 90% of patients experience arrhythmia, especially in the first 48 hours following the attack. If arrhythmias persist beyond this period, they require urgent intervention. Managing stress and anxiety can help reduce these risks.
- Acute heart failure: This complication is common within two weeks of the attack, particularly in the case of recurrence or pre-existing chest pain. Symptoms include low blood pressure, rapid weak pulse, and excessive sweating. If left-sided heart failure occurs, patients may experience severe shortness of breath and rapid heart rate with pulmonary edema.
- Embolism leading to stroke: Blood clots formed during the heart attack can travel to other organs, causing blockages in the blood vessels, leading to stroke or pulmonary embolism.
- Heart rupture: 10% of heart rupture cases occur in the second week following the attack, typically due to left ventricular rupture, which causes blood to spill from the heart lining, leading to circulatory collapse and death.
- Myocardial ischemia: 30% of heart attack patients suffer from secondary ischemia, manifesting as chest pain that requires emergency treatment like the acute phase. This complication is more common in long-term diabetes sufferers.
Late complications:
- Ventricular dilation: This occurs in 30% of cases and is associated with heart failure or aortic obstruction.
- Ventricular arrhythmia: An EF score under 35% combined with ventricular dilation requires the use of a pacemaker to manage arrhythmias.
- Shoulder-hand syndrome: This typically appears 6 to 8 weeks after the heart attack and affects the left shoulder and left hand, causing pain in the shoulder and wrist due to degeneration and fibrosis in the joint. Early physical activity after the incident reduces the risk of this complication.
- Neuropathic pain: Pain that starts in the chest and spreads to the surrounding areas, characterized by a dull ache and heaviness. This is often seen in people who are stressed, anxious, or physically and mentally exhausted. Psychological support and herbal remedies are recommended for treatment.
- Heart failure: Heart function declines significantly after a heart attack, rapidly progressing to heart failure.
- Pericarditis: 3-4% of patients experience this complication, which is marked by pain behind the sternum, worsened by breathing, physical activity, or coughing, and relieved when sitting or leaning forward.


2. Who is at risk for a heart attack?
The likelihood of experiencing an acute heart attack is higher among the following groups:
- Older individuals, men over 50, or women after menopause;
- People with hypertension, diabetes, or chronic kidney disease;
- Those with hereditary dyslipidemia;
- Smokers or those exposed to second-hand smoke;
- Individuals with a family history of early heart attacks or strokes (father, mother, siblings) before age 55 for men and before age 65 for women;
- People with autoimmune conditions like rheumatoid arthritis, systemic lupus erythematosus, psoriasis, or scleroderma;
- Those using stimulants like cocaine or amphetamines, which cause coronary artery constriction.


3. Diagnosis of Heart Attack
Heart attacks are usually diagnosed in emergency situations. Initially, the doctor will ask about the patient's symptoms and medical history. Then, blood pressure, pulse, and temperature will be measured, and a general heart health check will be conducted.
Tests to diagnose heart attacks include:
- Electrocardiogram (ECG): The first diagnostic test performed to detect heart attacks, which records electrical signals from the heart. Electrodes are attached to the chest, arms, and legs. The signal is displayed as a waveform, printed on paper, or shown on a monitor. An ECG of a heart attack can indicate whether the patient is experiencing or has a history of the condition.
- Blood tests: Certain heart proteins gradually leak into the bloodstream after the heart is damaged by a heart attack, called cardiac enzymes (troponin). Blood tests can check for these proteins (biomarkers of myocardial injury).
- Chest X-ray: Provides information on the condition and size of the heart and lungs, as well as other potential causes of chest pain.
- Cardiac ultrasound: Shows how blood moves through the heart and its valves, as well as the heart's pumping function. Ultrasound can help determine if any area of the heart is damaged.
- Coronary angiography: A long, thin tube (catheter) is inserted into an artery, typically in the arm, and guided to the heart. A contrast dye is injected through the catheter to make the arteries appear more clearly on the screen during the procedure.


4. How is Myocardial Infarction Treated?
Can myocardial infarction be cured? In reality, treatment for this condition is urgent in nature, but with a proper lifestyle, patients can still combat the potential long-term complications.
Methods of treating myocardial infarction include:
- Emergency Care:
- Patients experiencing chest pain should be rushed for emergency care, with treatment methods including:
- Oxygen therapy
- ECG monitoring
- Administering Aspirin: this drug helps to thin the blood and reduces the formation of blood clots
- Administering Glyceryl Trinitrate: this drug is placed under the patient’s tongue and helps relax blood vessels, allowing blood to flow through blockages, reducing the blood returning to the heart and lowering blood pressure
- Pain Management: Morphine is used to relieve pain and anxiety, reducing heart rate.
- Complications to monitor: arrhythmias, fluctuations in blood pressure.
- Patients experiencing chest pain should be rushed for emergency care, with treatment methods including:
- Coronary Artery Revascularization:
- Medical treatment: using clot-dissolving drugs like urokinase, streptokinase... During the emergency phase, anti-coagulant treatment is maintained using Vasopolis or Aspirin. Vasopolis is used for patients allergic to Aspirin or with stomach issues.
- Surgical treatment: a catheter is inserted through the femoral artery into the coronary artery to remove the clot and open up the artery, sometimes with a stent to keep the artery open.
- Coronary Artery Bypass Grafting:
- Coronary bypass surgery: This procedure is performed to restore blood supply to the heart during a blockage crisis by bypassing the obstructed artery using a graft.
- A vein from the leg is used to connect the aorta to the coronary artery beyond the blockage.
This treatment method is highly effective in most cases, with a success rate over 95%. It is performed by experienced cardiovascular specialists at Mytour, such as Dr. Lương Võ Quang Đăng - Cardiologist and Head of the Internal Medicine Department at Mytour International General Hospital Phu Quoc. Dr. Trần Quốc Tuấn, with 12 years of experience at Vĩnh Long General Hospital, Gia Định People's Hospital, and Nguyễn Trãi Hospital, currently works as an emergency physician at Mytour International General Hospital Phu Quoc. The fibrinolysis technique is carried out with the support of advanced imaging diagnostic equipment to ensure patient safety.


5. Effective Ways to Prevent Myocardial Infarction
To effectively prevent myocardial infarction, you must adopt a comprehensive approach, including lifestyle changes, managing risk factors, and regular health check-ups, which involve the following:
- Monitoring blood pressure
- Controlling blood sugar levels
- Reducing bad cholesterol levels
- Developing a weight loss plan at home
- Following a healthy diet plan
- Exercising 3-5 times per week
- Limiting alcohol consumption
- Quitting smoking to effectively prevent myocardial infarction
- Ensuring adequate sleep every night
- Managing stress
- Following prescribed medications
- Treating underlying risk conditions for myocardial infarction
- Getting regular cardiovascular check-ups


6. Important Considerations for Living with the Risk of Myocardial Infarction
Living with the risk of myocardial infarction is challenging, but you can implement the following tips to improve your quality of life and reduce your risk of the disease:
- Follow your doctor's instructions: Always consult your doctor and strictly adhere to their treatment plan.
- Adopt a healthier lifestyle: Embrace healthy habits, reduce stress, exercise regularly, and maintain an ideal weight.
- Stay informed and updated: Continuously increase your awareness of the disease you are facing, and stay informed about the latest prevention and treatment methods.
- Regular health check-ups: Schedule regular cardiovascular health check-ups to monitor your risk and adjust prevention strategies.


7. What is Myocardial Infarction?
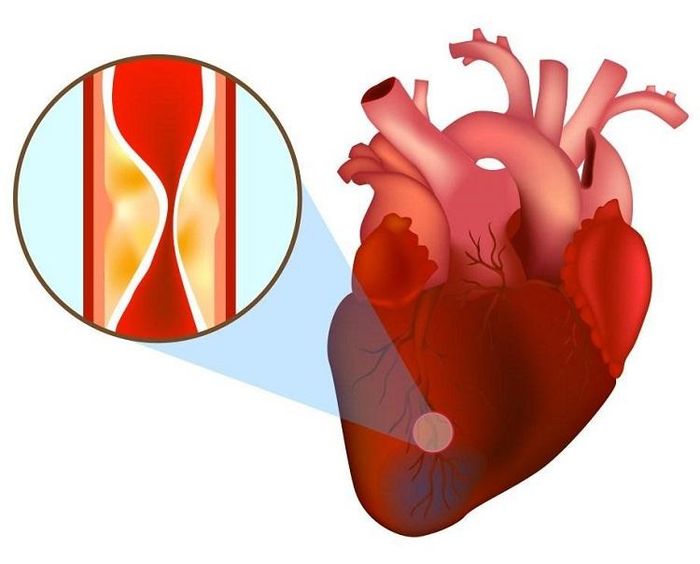
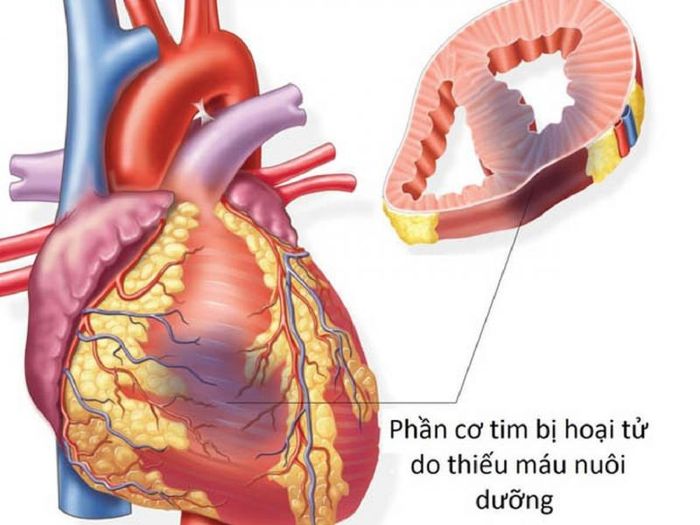
Myocardial infarction is the most severe complication of coronary artery disease and remains the leading cause of death in cardiovascular diseases today.
A heart attack occurs when the blood flow in the coronary artery, which delivers oxygen and nutrients to the heart muscle cells, is completely blocked. The part of the heart muscle that no longer receives adequate blood supply will begin to die. This is a medical emergency, and the patient can die rapidly if not treated promptly. Even those who survive often face a high risk of heart failure in the future.
In the United States, approximately 635,000 people suffer from a myocardial infarction, and about 300,000 experience a second heart attack every year. For every seven deaths, one is caused by heart disease, including myocardial infarction.

8. What causes an acute heart attack?
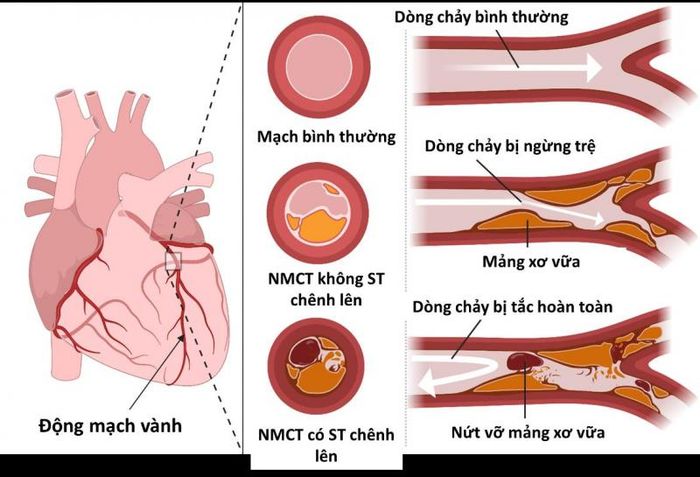
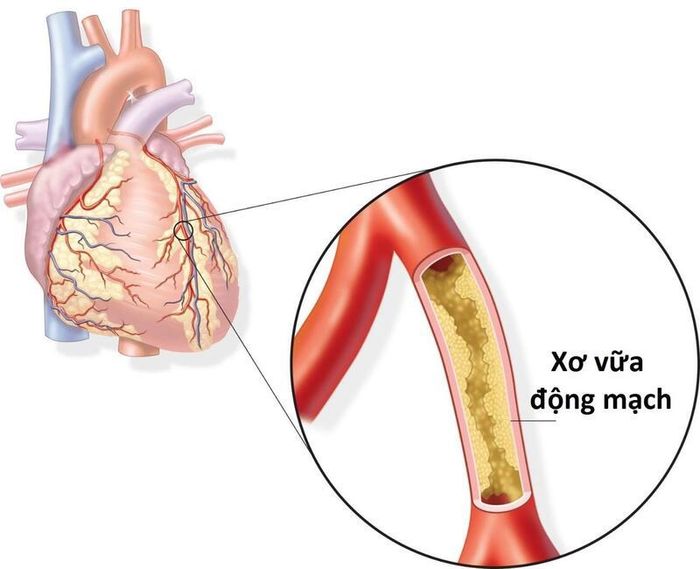
Due to atherosclerosis:
- This is the most common cause of heart attacks. When the body is exposed to risk factors for cardiovascular diseases in general and heart attacks in particular, substances like cholesterol, calcium, proteins, cell fragments, or inflammatory cells accumulate in the coronary arteries, forming plaques. These plaques are hard on the outside and soft on the inside. As these plaques harden, the outer layer cracks, and platelets are drawn to the damaged area of the coronary arteries, leading to the formation of blood clots around the plaque. These clots can block the coronary artery, cutting off the blood supply to the heart, depriving the heart muscle of oxygen and nutrients, causing it to die, and triggering heart attack symptoms.
Not due to atherosclerosis:
- This type of heart attack is rarer and usually associated with congenital abnormalities of the coronary arteries, such as malformations, fistulas, or abnormal origins. Since each coronary artery supplies a different part of the heart, when one branch is abnormal, the corresponding heart muscle area does not get enough blood, leading to heart disease.
- Infections of the coronary arteries, like Kawasaki disease, can promote inflammation and increase the likelihood of plaque formation, eventually leading to blood clot formation.
- Coronary artery spasm, unrelated to atherosclerosis, can suddenly cut off the blood supply to the heart, causing heart attack symptoms.
- Blood clots originating from other parts of the body, such as the lungs, kidneys, or brain, may travel to the coronary arteries, causing heart attacks.
Other causes of heart attacks include:
- Secondary coronary artery embolism.
- Primary coronary artery spasm.
- Congenital coronary artery defects: Some individuals have congenital coronary artery abnormalities, leading to obstructed blood flow to the heart.
- Ischemia caused by drug use (e.g., cocaine, ephedrine, amphetamines).
- Previous coronary artery trauma.
- Factors increasing oxygen demand: Conditions like hyperthyroidism, excessive exertion, and fever can increase the heart's oxygen demand, resulting in a heart attack.
- Factors decreasing oxygen supply: Severe anemia or other conditions that reduce oxygen supply to the heart can cause a heart attack.
- Arteritis: Inflammation of the arteries can lead to spasm and a heart attack.
- Aortic dissection: A dangerous condition that can affect blood flow to the heart.
- Acute lung diseases: Certain acute lung diseases can lead to oxygen deficiency in the blood, contributing to a heart attack.
9. How to identify a heart attack?
An acute heart attack occurs when a patient experiences specific signs such as intense chest pain, often felt like suffocating pressure behind the breastbone, in front of the heart, and radiating to the left shoulder, left arm, even extending to the little and ring fingers. The sudden pain usually lasts more than 20 minutes and does not improve with pain relief medications. The pain can spread to the neck, jaw, shoulder, arm, and even the back.
However, some patients may experience minimal or no pain at all, especially those with diabetes, high blood pressure, or after surgery.
Other symptoms may include excessive sweating, difficulty breathing, palpitations, nausea or vomiting, memory loss, pale skin, and cold extremities...